

Everything You Need To Know About The Hantavirus Boat
A deep dive into the current state of the MV Hondius hantavirus outbreak, the timeline of events, the virus itself, and the global response to the situation.

As you’ve probably heard by now, a Dutch-flagged expedition ship called the MV Hondius and the world at large are currently on high alert, as what was supposed to be a scenic voyage from Argentina to the Canary Islands turned into a floating quarantine zone due to a hantavirus outbreak.
I want to be clear outright that as of Thursday, May 7, the World Health Organization (WHO) currently assesses the global risk as low, and has said outright that this is not a pandemic.
However, in the event of an escalation, the U.S. is uniquely vulnerable because we’ve effectively unplugged our early warning systems, which we’ll get into.
This is nowhere near the level of alarm as the COVID-19 outbreak as of right now, but similar to that pandemic, there is a lot of hysteria and misinformation surrounding these kinds of outbreaks, so I’m going to break the situation down in detail for you.
The Uptake is a reader-supported publication.
To receive new posts and support the free outbreak reporting and deep healthcare analysis I do here, consider becoming a paid subscriber.
The Timeline of Events
April 1, 2026: The MV Hondius departs Ushuaia, Argentina, with 147 passengers and crew.
April 6: The first passenger (an adult male) begins showing symptoms—fever, headache, and diarrhea.
April 11: The first passenger dies on board. At this point, nobody knows it’s hantavirus.
April 24: The ship stops at Saint Helena. The first victim’s body is removed, and his wife disembarks. It was also recently discovered that 26 other passengers disembarked from the ship on April 24. Some are Americans. None are known to be sick, and these were apparently planned disembarkations, not medical evacuations. Seven of these people have already returned to the U.S., and states are working to track them down for testing and monitoring.
April 26: The wife dies in a Johannesburg hospital after falling ill during her flight from Saint Helena.
May 2: Lab tests in South Africa confirm hantavirus. The ship anchors off Cabo Verde, but the government refuses to let passengers disembark.
May 3: A third passenger dies on board. The World Health Organization (WHO) is officially notified of a cluster of severe respiratory illnesses.
Current Status
At least one of these has been officially sequenced as the Andes virus (ANDV), which confirms our fears about the potential for person-to-person spread.
The death toll remains at three: a Dutch couple and one German national.
Yesterday, the most critical patients were evacuated from the ship off the coast of Cabo Verde via air ambulances and sent to specialized isolation units in South Africa and Europe.

A British man, 56 (now identified as Martin Anstee), a Dutch crew member, 41, and a German national, 65, were sent from the MV Hondius to the Netherlands for treatment, officials said.
Two out of the three evacuated passengers have arrived at a Netherlands hospital for treatment, while the third was on board an evacuation flight that has been delayed.
The ship left Cape Verde yesterday and has begun a three-day journey to the Canary Islands, heading toward Tenerife, the largest of the islands, where health authorities are bracing for its arrival.
As of right now, it’s estimated to arrive at the port of Granadilla in the early hours of Sunday, May 10.
It’s been denied entry by several ports, and the President of the Canary Islands, Fernando Clavijo, has publicly objected to the docking, but the Spanish central government and WHO are pushing forward.
The Offboarded Passengers
The biggest concern right now is the passengers who disembarked (for planned, non-medical reasons) on April 24.
Because those two dozen people from 12 countries left the ship at Saint Helena, they are now scattered across the globe and may or may not be infected, which could lead to more widespread, unenclosed exposure if left unattended.
6 of these passengers were American.
Here’s the current status of what we know about them now:
U.S. Residents: Health officials are currently monitoring residents who returned to Arizona, California, Georgia, and Texas.
The Georgia Update: At least two Georgia residents are officially under watch.
Isolation Protocol: These individuals are being told to monitor their health for up to eight weeks, which is the most cautious window for hantavirus incubation.
What Is Hantavirus & How Does It Spread
Think of hantavirus as the ultimate “don’t breathe the dust” warning.
It’s a family of viruses primarily carried by rodents. In the Americas, it has a deadly reputation because the strains here usually cause Hantavirus Pulmonary Syndrome (HPS), which triggers a deadly immune response that causes capillaries to leak, essentially filling your lungs with fluid.
Whether a hantavirus infection leads to HPS (Hantavirus Pulmonary Syndrome) depends almost entirely on the specific strain and the region where it is found:
In the Americas: The strains here almost always present as HPS (also referred to as HCPS). While human infection is far less common than in other parts of the world, these strains are specifically known for causing severe respiratory illness.
In Europe and Asia: Hantaviruses in these regions typically cause Hemorrhagic Fever with Renal Syndrome (HFRS), which primarily attacks the kidneys rather than the lungs. These infections are far more frequent, accounting for 10,000 to over 100,000 cases annually, but most hantavirus infections globally do not progress to the severe stage of HPS.
The European and Asian strains have a much broader range of severity. The death rate for HFRS varies from less than 1% to about 15%, making them significantly less lethal on average than the pulmonary versions found in the Western Hemisphere.
In the Americas, hantavirus infections are far deadlier because HPS is far deadlier, and these strains almost always cause HPS. The two main strains are the Andes virus and the Sin Nombre virus.
Andes virus fatality rates commonly range from 30% to 50%, and fatality for the Sin Nombre virus is approximately 36% to 40%. It’s really bad.

Luckily for most cases, hantaviruses are dead-end infections. Humans generally get it from breathing in aerosolized dried urine, droppings, or saliva from mice, but they typically can’t pass it to another person.
The terrifying exception is the Andes virus, which is the only hantavirus known to spread person-to-person through close contact. Unfortunately, the Andes virus is the strain that was identified on the MV Hondius…
If you’re wondering how it got there, the ship started its journey in Argentina, where the Andes virus is endemic (aka native) and has seen a geographic shift and increase in cases during the 2025–2026 season.
Investigators now suspect the outbreak may have started when a Dutch couple went on a birdwatching trip to a landfill site in Ushuaia, Argentina, before boarding. Landfills are high-density rodent areas, which would explain the initial exposure.
TLDR: most hantaviruses are hard to catch, and most do not progress to the disease that is the most fatal, however the one on the ship is unfortunately the kind that is much easier to catch and is almost always fatal.
Since tragically that’s the one that we’re talking about, let’s get into how this specific virus works.
The Andes Virus
Again, the Andes virus’s claim to fame is that it’s the only hantavirus known to spread directly between humans.
It usually requires close, prolonged contact. Think of it like a family-and-friends virus rather than something that spreads through a casual handshake.
Here’s everything we know about the specific culprit virus strain.
How It Works
It can be found in saliva and respiratory droplets, meaning if you’re sharing a cabin on a ship or taking care of a sick family member, you’re in the splash zone.
It’s most contagious during the prodromal phase, which is that early window when the person just thinks they have a nasty flu but hasn’t reached the emergency stage yet.
That means if you think you have the flu and are walking around interacting with people, trying to push through it, you’re an infection risk (please stop doing that, everyone).
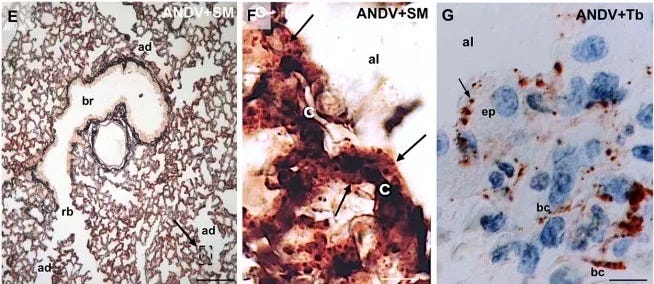
The Hantavirus Pulmonary Syndrome (HPS) that the Andes virus almost always causes is horrifically efficient at killing.
The virus doesn’t actually destroy your lung cells like many respiratory infections. Instead, it triggers a massive immune overreaction (called a cytokine storm). This causes your capillaries to become leaky.
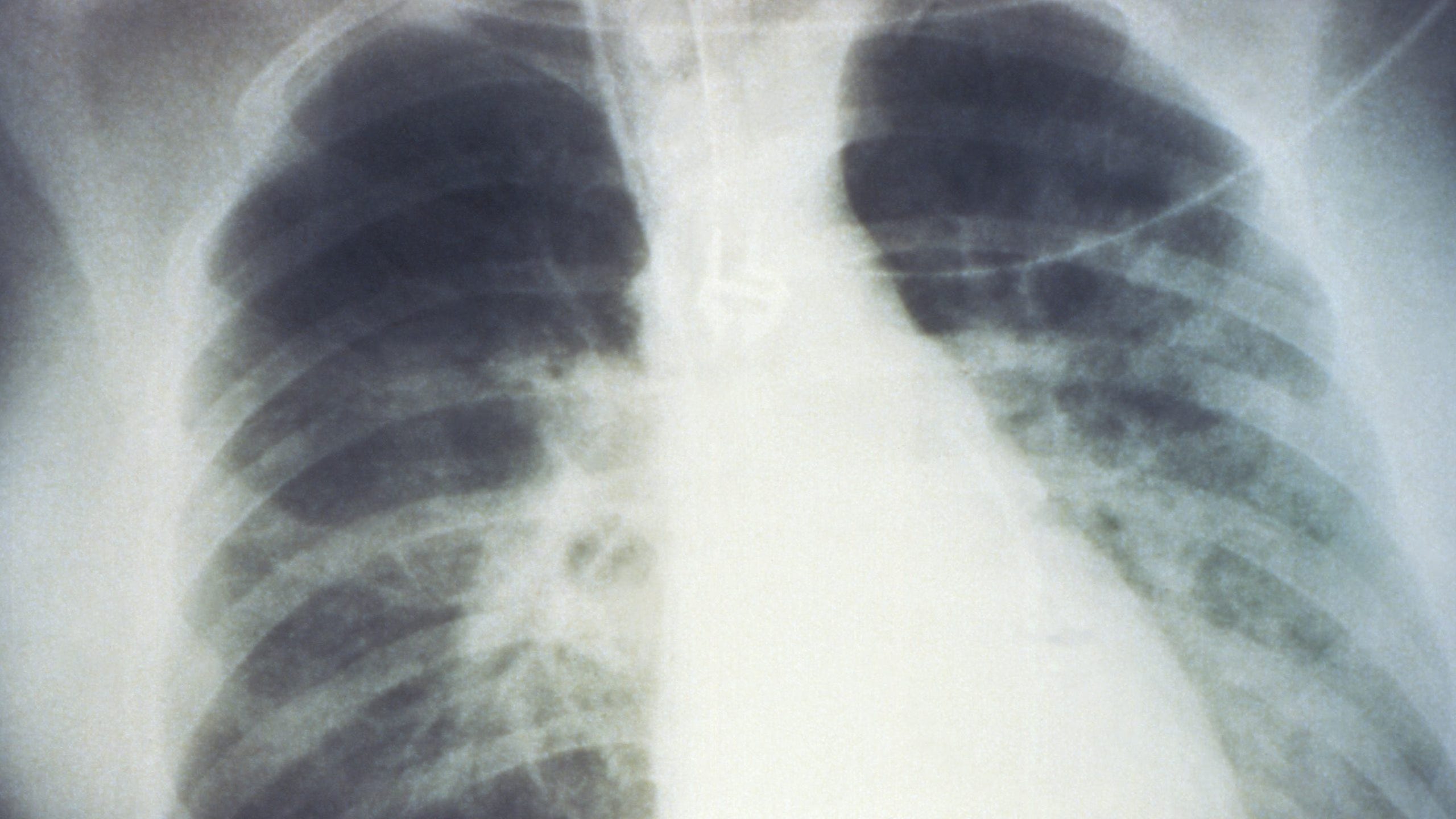
What this looks like in practice is really ghastly. Plasma from your blood leaks directly into your lungs, meaning you’re not “sick” in the traditional sense; you’re essentially drowning from the inside out.
This is why it’s so incredibly lethal, with a mortality rate of around 35–40%, and once the respiratory distress starts, things go south fast, often within 24 to 48 hours.
Where It Comes From
Its natural home is the long-tailed pygmy rice rat (Oligoryzomys longicaudatus). These little rascals are cute but carry the virus in their saliva, pee, and poop.
It was first identified in 1995 in Argentina (which is why it’s named after the Andes mountains). A year later, a famous outbreak in El Bolsón, Argentina, proved for the first time that humans could give it to each other.

Since the MV Hondius started its journey in Argentina and visited remote South Atlantic islands, it’s likely someone encountered the virus there—either by breathing in the rat's pee or through close contact with someone who did.
Can We Treat It?
Unfortunately, we don’t have a vaccine or a specific antidote for the Andes virus yet.
Treatment for the Andes virus is all about supportive care. Doctors basically put you on a ventilator or an ECMO machine (which breathes for you and cleans your blood) and hope that your body can fight it off.
However, there’s some cool research into using convalescent plasma—taking the blood of people who survived and giving their antibodies to sick patients—which has shown some success in lowering the death rate.
When it comes to preventing its spread, it’s dead serious.
Because it can jump from person to person, labs have to handle Andes virus with Biosafety Level 4 (BSL-4) precautions. That’s the highest level of security, the same stuff used for Ebola.
A bit of good news, though, it was reported today that a team led by the University of Bath has been developing a hantavirus vaccine for the past two years. They hope to complete clinical trials in the next three to five years.
What The World Is Doing About This
The global situation has shifted from containment to active management as of today, Thursday, May 7. While the WHO is working hard to keep the public calm, the logistical response is ramping up significantly.
Here is the updated breakdown of how nations and organizations are handling the situation:
WHO & Africa CDC: Managed Repatriation Strategy
The WHO has taken a lead role in shifting the ship’s status from a pariah vessel to a managed medical site.
In a major press conference today, WHO officials (including Maria Van Kerkhove, PhD, WHO’s director of epidemic and pandemic preparedness and prevention) reiterated that this is not the start of a pandemic.
They emphasized that while the Andes virus is scary, it is not an airborne respiratory virus like SARS-CoV-2; it generally requires close, family-style contact to spread.
The WHO has also shipped 2,500 hantavirus diagnostic kits to laboratories in five key countries to ensure that any new cases are caught instantly.
Spain & The Canary Islands: The Reluctant Host
The ship is currently steaming toward Tenerife, despite vocal protests from the President of the Canary Islands.
The forthcoming arrival has also caused significant anxiety among residents and local officials, reviving fears of Covid-era quarantines, especially as the archipelago's economy relies heavily on tourism
Upon arrival, Spain will implement a tiered isolation protocol. Spanish nationals will be quarantined in Madrid, while international passengers will be immediately repatriated to their home countries via secured transport.
SA & The Netherlands: High-Security Treatment
These nations have stepped up to handle the most critical front-line cases.
The National Institute for Communicable Diseases in South Africa was the first to sequence the virus, proving it was the Andes strain. They are currently managing the care of those who fell ill after disembarking early.
A second patient has officially tested positive at a Dutch hospital. The Netherlands is also serving as the primary hub for the ship’s operator, Oceanwide Expeditions, to coordinate family notifications.
How Prepared Are We In The U.S.?
Again, this outbreak is not a pandemic given the transmission methodology, but given that this event has sparked COVID-era flashbacks and anxieties, it’s important to contextualize how our ability to handle these situations has been impacted.
As you can expect, if you’ve been following The Uptake or recent news on how the Trump administration has handled healthcare, we’re extremely ill-prepared.
Major Concerns
There are several recent factors that would greatly affect our ability to monitor disease spread and coordinate a response.
In January 2025, the U.S. officially withdrew from the World Health Organization (WHO). Because of this, the U.S. isn’t getting the same real-time data or resource-sharing as other countries, and we are already preventing CDC employees from co-authoring papers with WHO staff, essentially leaving us flying blind while everyone else is in a group chat.
On top of that, the 2026 FIFA World Cup is set to start in just a few weeks across 11 U.S. cities. With millions of international travelers arriving, our lack of coordination with global health bodies is a massive red flag.
After the pandemic fatigue of the early 2020s, many domestic surveillance programs were scaled back. Health departments in states and localities nationwide are facing severe budget reductions and layoffs.
If the Andes virus starts jumping between people in a crowded stadium, the U.S. might not detect it until the ICUs are already full.
Lastly, the Trump administration’s recent gutting of fundamental American health infrastructure poses one of our greatest setbacks.
A System in Crisis
The situation at the CDC is pretty dire. The Trump administration has implemented sweeping changes to how the U.S. handles public health, creating a perfect storm for something like the Andes virus to slip through the cracks.
When it comes to how much has been cut, the numbers are staggering. The FY 2026 President’s Budget proposes reducing the CDC’s budget by a massive 53% from FY 2024 levels. These cuts were surgically targeted at the exact tools needed to stop an outbreak:
Global Health Security: This department—which tracks overseas outbreaks before they reach our borders—is among the 61 CDC programs facing elimination, with impacts on global immunization and HIV/AIDS prevention.
Staffing: Proposed reorganizations would reduce public health staff positions by 16%, leaving high-level leadership positions vacant. We’ve essentially lost the institutional memory of how to handle a respiratory crisis.
Now that passengers from the MV Hondius have landed in the U.S., the real-world impacts are concerning.
Because we withdrew from the WHO and cut global surveillance, we aren’t getting the same raw data feeds from Cabo Verde or Argentina that other countries are. In an outbreak, every hour counts.
The administration is also using budget eliminations to reset the balance between federal and state responsibilities. This means states would end up competing for limited resources like ventilators or ECMO machines rather than having a federal command center.
Again, based on current knowledge of the virus’s spread, the risk of a large-scale outbreak remains low.
However, the machinery of our healthcare response was in place to ensure we were prepared if things escalated or another outbreak occurred.
The biggest takeaway from this situation is that outbreaks will hit again, and if that machinery is not fixed, the consequences could be dire.